|
|||||||||
| home | learn about your condition | about somatics | site contents | store | testimonials | about Lawrence Gold | get professional training | contact | |
|
||||||||||||||||||||||||||||
|
|
by Lawrence Gold
|
|
|
Doctors and patients commonly regard sciatica as difficult to cure. When you take one of the approaches most commonly used: drugs, stretching (including an inversion table), manipulation, surgery, it does seem difficult to cure. Your final relief may take forever. None of the usual approaches gets at the underlying cause, so relief is partial, temporary, or may never occur to the point that you are free of sciatica and can move freely.
This article explains the underlying causes in understandable language and presents an alternative, effective approach -- one that can end sciatica in a few weeks -- but there is a catch: you have to do the work. YOUR CHOICE of APPROACHThere are two ways you can approach sciatica: as a "consumer" of care and as a "do-it-yourselfer".A "consumer" expects to pay someone for their expertise and have them "do it for them". "Expertise" includes the "expertise" of the pharmaceutical companies. The consumer turns to experts, or to their products, to "fix" him or her. The consumer doesn't want to have to understand; that's what s/he pays the expert for. A "do-it-yourselfer" learns about the condition to the point of arriving at an understanding of its cause that makes sense -- and then does what it takes to get the required result. With sciatica, you can't be a consumer and get the relief you seek. Sciatica doesn't work that way; it's not that kind of condition. It's not caused by something external, so that you can do or take an "external" approach and fix it. It's caused by something your body is doing to itself. This article explains what your body is doing to itself (really, what you are involuntarily and unconsciously doing to yourself) to cause the pain and what you can do -- not to counteract it, but to cease doing it (it's not restricting movement or "neutral spine position", but something entirely different). When you do, the pain fades out and everything is all right, again. If you are going to get free of sciatica any time soon, you're going to have to understand what's going on in you and be a do-it-yourselfer. Standard therapeutics won't do it. If you doubt me, continue with the "consumer" way of operating until you see its failure. Then, you may come back here, learn what you need to learn, and become the do-it-yourselfer you need to be to end your sciatica. |
||
|
The Three Biggest Mistakes Made
by People Trying to Get Out of Pain
Listen to Someone Getting
|
|
|
Because some people think they have sciatica -- when actually, they have another condition that mimics sciatica -- I'm going to teach you to distinguish sciatica from other conditions.
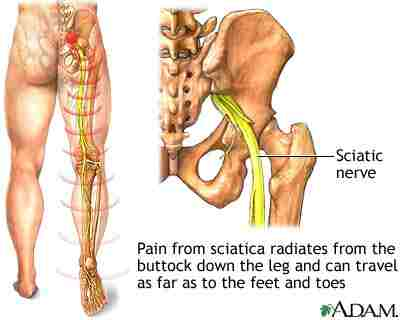
Typical sciatica starts at the buttock (usually one side, only) and may extend down the back of the leg as far as the foot. Sensations may include numbness, burning, or the feeling of a hot cable going down the buttock, under the "sit-bone", down or back of the leg. If, when rubbing these places, you feel like you can't affect the pain, it's nerve pain (sciatica). If rubbing brings relief, it's muscular pain, not sciatica.
If you have pain going down the front of your leg, you may have a muscle spasm of the front thigh muscles; if pain down the side, it may be ilio-tibial (IT) band syndrome or a twisted sacrum (sacro-iliac joint dysfunction/SIJD); if skin numbness or burning down the front, it's likely a twisted sacrum.
|
The Root Causes of SciaticaThe two most common causes of sciatica are nerve compression caused by tight muscles in the back and waist (common sciatica) or buttock (piriformis syndrome). More, below.The muscles of the back are like the string of an archer's bow and the spinal column, like the bow, itself. As the tension of a bowstring causes the bow to bend, tension of the back muscles causes the low back to bow forward (swayback). Tension of the waist muscles at the side causes side tilt. The combination of swayback and side-tilt traps and puts pressure on the sciatic nerve where it exits the spinal column. Result: sciatica. Muscle tension of this sort persists despite efforts at relaxation or muscle manipulation. Brain-conditioning (muscle/movement memory) keeps muscles tight. Because brain-conditioning overrides efforts at relaxation or manipulation, sciatica persists or returns shortly after massaging or manipulation. For that reason, sciatica tends to persist despite therapeutic efforts and people find it difficult to correct. It's a matter of approach and the standard approaches seem to take forever. Another approach brings rapid and durable relief: change the brain-level conditioning; change muscle/movement memory. This approach works faster and more effectively than approaches that use manipulation or common relaxation techniques. It's also comfortable to go through. |
Personal Attention Mentoring
|
The brain-level conditioning (muscle/movement memory) that causes sciatica typically forms from an injury to a leg or foot, or a hard fall). The pain of injury causes a cringe response that affects the back, waist muscles, and/or buttock. A side-tilt forms (see photos, below, showing "before" and "after".)
To end sciatica involves ending that cringe response. The techniques of clinical somatic education do that, quickly and efficiently. No manipulation is involved; it's done entirely by learning to control and relax the muscles and movements that cause sciatica. Symptoms disappear as that control improves -- again, fairly quickly.
|
|
The reason I'm telling you about all four types is that if you have a ruptured or herniated disc, you should not do the approach shown, here.
See the path of the sciatic nerve in the illustration.
The sciatic nerve has roots that exit the spinal cord at, L3 - L5, the lowest three vertebra of the lumbar spine (low back). The nerves pass in front of the sacrum (central bone of the pelvis) and then out, through the buttocks and down the backs of the legs to the feet.
|
|
|
Common SciaticaCommon sciatica results from a combination of excessive swayback (lordosis) and side-tilt (scoliosis) -- both muscularly induced conditions maintained by muscle/movement memory.The combination of swayback and side-tilt reduces the space through which the nerve roots pass and squeezes them ("nerve impingement" or "pinched nerve"), which causes sciatica.
Piriformis syndrome comes from contraction of the piriformis muscle of the buttock (usually one side, only), through which the sciatic nerve passes in some people, and around which it passes, in others. Mere passage through the muscle is not enough to cause symptoms, but if the piriformis muscle is too tight for too long, sciatica results. Although both common sciatica and piriformis syndrome may take a while to develop, they appear suddenly and they both disappear very quickly, once the muscular cause ends.
Because the method described, here, clinical somatic education, works quickly, surgical intervention is properly a last resort after trying clinical somatic education. You may get an MRI scan to rule out disc rupture or herniation before starting.
Ruptured discs, and their precursor, herniated disc(s), are delicate conditions that require special care. Refrain from somatic education exercises because, as gentle as the exercises are, you may not be able to work gently enough and may endanger your discs. You should do somatic education exercises if you have a herniated disc only under the in-person guidance of a certified clinical somatic educator. You should not do somatic education exercises, at all, if you have a ruptured disc because it would be wasted effort; get any needed surgery, beforehand and get somatic education to prevent other discs from herniating or rupturing. Even more rare than disc herniation or rupture is a condition in which the holes (foramena) through which the nerve roots exit the spinal column, and/or the spinal canal, narrow because of bone growth (stenosis). Generally, these last two forms of sciatica are surgical situations, although some therapists are said to be able to use "MacKenzie Exercises" to cause the re-uptake of extruded disc material and so alleviate symptoms. Even if surgery is successful, one must still deal with muscular contractions that are virtually always the cause of sciatica developing. |
CONVENTIONAL TREATMENT OF SCIATICAConventional, non-surgical treatment of sciatica may consist of five approaches:
Of these approaches, the first three do nothing to address the cause of sciatica (described, above). The fourth approach, manipulation, has the right idea -- free the tight muscles -- but can't work. Manipulation doesn't change muscular conditioning, so muscles re-tighten and sciatica symptoms reappear or never disappear. The fifth approach, strengthening, completely misses the mark. Sciatica comes from muscles that are too tight, so strengthening takes things precisely the wrong direction: muscles go into stronger contraction.
|
|
|||
|
Stretching should never be done because trapped nerves lack their full elasticity and are vulnerable to damage from stretching. Surgical Approaches
MicrodiscectomyMicrodiscectomy means cutting or shaving away part of a disc that is pressing/impinging upon the sciatic nerve.While microdiscectomy may seem "mechanically logical", it has two major faults:
Lumbar laminectomy involves removal of the part of vertebrae that can be seen on the back and felt by touching. Not only does laminectomy fail to address the underlying cause of sciatica; it also triggers muscles in the region to tighten further in reaction to the trauma of the surgery -- and their being too tight was the problem to begin with. If any benefit results, it comes not from the surgery but from the therapy that follows.
The poor results of such approaches to stopping sciatica speak for themselves. How do I know? I've had clients come to me for help with sciatica who have had a laminectomy. Yes, somatics worked, for them.
Where tight muscles put pressure on the sciatic nerve, the direct remedy is to free those muscles. "Free" means, "slacken" -- which maintaining full function.
Since brain-conditioning is behind most sciatica, the direct approach is to recondition control of the involved muscles. Somatic education uses a brain-level response related to yawning that can be used to free muscles anywhere in the body. The video, Pandiculation, explains.
|
||||
|
As muscles relax, (1) swayback decreases, and (2) side-tilt straightens, and pressure comes off the sciatic nerve. Pain fades, nearly immediately. Pain can be completely extinguished, this way, and full function restored. |
||||
|
[AUTHOR'S NOTE: My mother had piriformis syndrome in 1989. I directed her to the developer of this approach, Thomas Hanna, Ph.D., who practiced within driving distance. This was before he trained me. She came back, that afternoon, without the sciatica and with the words, "You've got to learn this work!"] Relief of either of these forms of sciatica occurs within moments of the relaxation and, for all intents and purposes, is permanent, since muscle/movement memory has normalized. For any therapeutic approach to be effective with sciatica, it must normalize muscle/movement memory, which the underlying cause of sciatica. Clinical Somatic Education leaves you with no movement restrictions or need to maintain a neutral spine position; you may comfortably and safely move in any direction and, if your discs are sound, do any activity, whatsoever, safely. Click Somatic Education Exercises for Neuromuscular Stress and Pain, to learn more about a program that delivers the results described, here.
|
||
|
Bookmark this page? [CTRL]+[D] (windows) | Bookmark on |
||
![]()
Get started, for free.as adapted to Comforting Your S-I Joints
FULL PROGRAM:
Lessons 1 - 4 specifically effective for sciatica | 1 - 4 weeks
Click here to have me work with you, in person.
LIFETIME SATISFACTION REFUND GUARANTEE
|
|
The Institute for Somatic Study and Development
Lawrence Gold, certified Hanna somatic educator
This page may be reproduced freely in its entirety.
|